
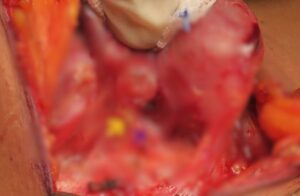



We routinely do locally advanced thyroid surgeries with neck nodal enlargement, tumour infiltrating into surrounding structures and extension into chest

Huge thyroid mass extending into chest. Chest bone is split to remove the mass.
RADIO IODINE THERAPHY– Advanced cancers of thyroid (papillary and follicular) require post surgery Radio iodine theraphy to ablate metastatic disease.
Well placed neck scar for thyroidectomy heals well and align with neck folds so that it is not visible obviously after 4 months of surgery. Steps taken to produce a fine thyroidectomy scar
1) Incision placed in natural neck fold.
2) Sub-cutaneous suturing done with absorbable sutures so that scar is thin.
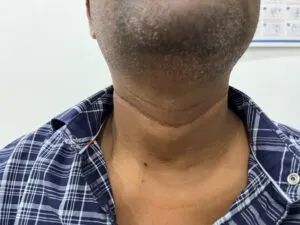
This patient underwent thyroidectomy with neck dissection on both side of neck with 10 cm incision which is well healed .
Another fine thyroidectomy with neck dissection scar for cancer of thyroid.

Robotic thyroidectomy can be done from mouth called trans oral thyroidectomy vestibular approach(TORTVA) or from behind the ear called retro auricular approach.
In TORTVA three small incisions are made in lower lip for robotic arms to enter into neck and thyroid gland is removed from mouth .Excellent cosmetic results with no visible scar in neck.
In post aural robotic thyroidectomy incision is given behind hairline behind the ear for access into neck. So scar is actually concealed and not visible in neck.
1)Non cancerous lump in thyroid
2)Size less than 4 cm
3)No involvement of neck nodes.
ADVANTAGE – No visible scar in neck
DISADVANTAGE-Increased surgery time
-Expensive when compared to open surgery


We are experienced in management of recurrent nerve injury. Voice change can be treated with THYROPLASTY and injection laryngoplsty.
LASER CORDECTOMY is done in patients with injury to both side recurrent laryngeal nerves with breathing difficulty .

